Less than six months into his tenure at Care New England Health System, Dr. Michael Wagner has clear ideas on how he wants to lead Rhode Island’s second-largest hospital group.
Charged with leading the recovery of a system strained by the aftermath of the COVID-19 pandemic and systemwide financial challenges, short-term financial viability is the main priority, he says. Every other discussion – including that of mergers and alliances – will have to wait.
Care New England and Lifespan Corp. both made headlines last year for their latest failed merger attempt, which some saw as the only viable long-term solution to the financial troubles. But to Wagner, merging is only one of the solutions – and not one he is thinking about at the moment.
“Does merging with somebody else help to provide more capital and stability to get access to capital?” said Wagner, who was previously chief physician executive of Tufts Medicine, a health system in the Boston area. “The answer is yes. But we’re not at that level of performance. We’re really back at getting to a positive operating motion. That’s our first order of business.”
What were your first priorities coming in and how much of it did you get started on already? One of the benefits of being somebody who’s run a health system in the role that I played at Tufts Medicine [Inc.] as the interim [CEO and president] in ’19, [and] being the CEO for Tufts Medical Center for five years, is that I’ve done this before. So I can walk in and rapidly evaluate and say, where are there areas for us to be addressing? And the financials were No. 1. And the reason was in large measure because of 2022 being such a difficult year financially, not just for Care New England but for all health care systems in the U.S. And relatively, Care New England performed better than most organizations in 2022.
There were signs of improvement in CNE’s performance [last quarter]. What do you think caused that, especially coming out of a difficult 2022? There’s considerable improvement at Women & Infants [Hospital]. And so they saw the greatest improvement at the operating unit level, so some pretty dramatic improvement. And that had lots to do with volume coming back, they have a surgical platform and I think just incredible leadership on the part of Shannon Sullivan. [Editor’s note: Nearly 1,400 unionized caregivers at Women & Infants voted no confidence in the hospital’s management on March 27, citing years of unheard grievances among the reasons for the vote.] … At the corporate level, there’s about $160 million in the budget. … The overhead in the corporate line was actually a pretty dramatic improvement in terms of reduction. That’s a good thing because we’re spending less money on things that aren’t in the direct line of patient care. … Then lastly Integra, our population health company that has done a great job at taking and managing risk for patients with the managed care companies, also had a financial improvement as well over the last year. … One of the benefits of developing a system … is the concept of stability. Because when you have not-for-profit [units], not every year all of them achieve their margin targets. But if you actually have them under a system umbrella, you provide protection on a year-by-year basis that some might do better, some might do worse. But by being together, you create greater stability. And that’s what Care New England has provided. There’s no question that merging and becoming part of a larger system creates stability, organizational stability, and I think that CNE coming together years ago created stability for each of the [units] that’s underneath that.
[caption id="attachment_434954" align="alignright" width="500"]

BRIGHT SPOT? Dr. Michael Wagner, CEO and president of Care New England Health System, says Women & Infants Hospital has made strides to improving its financial performance, although unionized employees at the hospital recently voted no confidence in its managers.
COURTESY CARE
NEW ENGLAND
HEALTH SYSTEM[/caption]
How much do you focus on individual pieces under the CNE umbrella? One of the things we instituted when I came on board in December was a rigorous monthly business review. So we sit down … with the operating unit presidents. … And we have a detailed conversation regarding their performance. The first thing we talk about is quality. Are they achieving their quality objectives? And are there any quality issues that we need to be addressing? And then we get right into the business of the organization, including their bottom line, how they’ve done, whether they made a margin or not, and then their revenue drivers and their cost drivers. Because ultimately what we want to see is a margin. … It’s our expectation that every one of our business units is generating a margin. I did it when I was at Tufts Medical Center. We went through a financially difficult time, and it turned the organization around. And I truly believe that organizations, especially through the pandemic, have lost that focus [on margin] because they were in such an emergency management mode. Now we’re moving into a more stable mode. Using standard techniques like monthly business review has become an important way to focus the organization and we’re already starting to see, I think, the positive impact of that.
What is the outcome you want to achieve? We’re at a negative margin because of our losses. We need to generate a positive margin. … If we’d got to a stable 4-5% as a run-rate perspective, and we could get there by the end of this calendar year, I would feel like we were making huge progress. That’s a pretty audacious goal. But that’s the one that I kind of laid out for people.
What are the steps you’re taking and what are the main things that stand in the way of the goal? You can’t live off of nonoperating gains. Health care organizations need to generate an operating bottom line. … Many organizations make the mistake that they call a consulting firm in, they call in one of the big firms … I don’t think they work because it deflects the ownership of who actually is driving this. So the first is the understanding and recognition that the executive team and the board own the responsibility for the financial turnaround of the organization. That’s probably the most important piece of this, and our team owns our current financial situation and the turnaround for the organization. So what are the levers that the team pulls together? First is standard in the playbook: you look at your cost structure. … We’re not looking at making changes that have a direct patient impact. Our goal is to protect the front line. … We canceled several consulting engagements of companies that were working with us because we really looked at what they were delivering and said, “It’s not delivering value, so we need to take you out.” So we’ve gone through that and the teams are going through a nice review from a cost-cutting perspective.
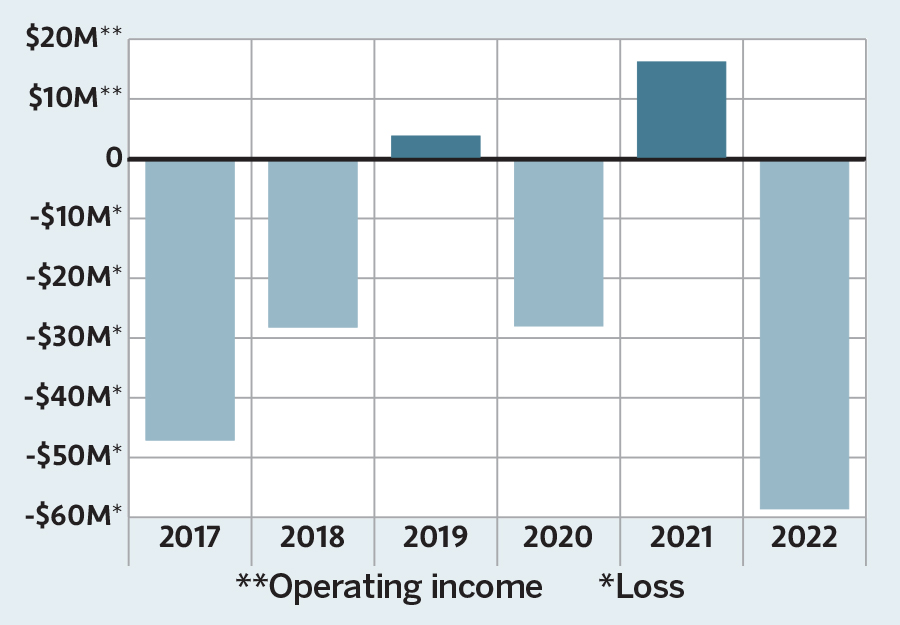
[caption id="attachment_434955" align="alignleft" width="456"]
AT A LOSS Care New England Health System has finished four of the last six fiscal years with a sizable deficit. In its most recent profitable year, 2021,
CNE and other health care organizations received a big boost from COVID-19 federal relief aid.
SOURCE: Care New England
Health System financial statements[/caption]
Does that include letting anyone go from the executive teams? We’re looking at that currently and I don’t have a number. But have we made some decisions about positions that we may not need? Yes.
But those would all be on the administrative side? Yes, the ones I’m talking about are in the administrative side. You look at your cost structure and you look at things that are discretionary spend that you can reduce. … You look at areas that we know are core to our business: the operating room and procedure platform at Kent [County Memorial Hospital]. … So [Dr. Paari Gopalakrishnan, Kent president and chief operating officer] is working with Melissa Murphy, our surgical chief down there, to look for ways to grow more surgical volume. … Same is true with Women & Infants, we’re focused on growth that is more profitable than other growth. … Some of the things we’re looking at is how we get reimbursed from the payer perspective.
The conversation about reimbursement comes up a lot. How much of a difference would it be for hospitals if we changed how hospitals get reimbursed under Medicaid? The general thing that I’ve heard … is that the [margins of hospitals in Rhode Island] have essentially been zero or negative over a very long period of time. And that’s just not sustainable. … It’s a combination of a couple of factors. One is the high Medicaid rate at the state level. [One-third] of the citizens of Rhode Island are on Medicaid. And Medicaid notoriously is the worst payer. … The payer structure here is not favorable for hospitals to actually make a margin.
If you look at the numbers of Kent … OK, their volumes are down and they’ve got to get volume back, especially in the surgical platform. OK, check. We’re working on that. There’s a plan with our surgeons and our chief surgeon there to do that. Cardiology, same thing. So that’s one: get volumes back and build those programs. Two is cost structure: are they structured correctly from a cost perspective and using their resources as efficiently as possible? … And then the third is the case-mix index. … If that number is not where it needs to be for an acute care hospital like Kent, the reimbursement for the hospital will not be commensurate with the cost structure of the hospital. … If we actually get these numbers where they need to be for a typical acute care hospital in the U.S., the numbers for Kent will actually be incredible. … Merging with somebody else doesn’t fix any of those things that I just said. If we were to merge with somebody else, it’s not as if magically those levers would change.
Do you think accessing capital will become a priority eventually, once CNE returns to a positive operating margin? Will a conversation about partnerships and mergers happen then? It will depend on what we’re able to achieve from an operating margin perspective. Now that we’ve got that first plate spinning on our operating margin performance and we have a plan, I want [CNE administrators] to lift [their] heads up a little bit and I want [them] to look out a year, two years, three years, five years. What are those things that we have on our roadmap that we need to start writing down that we need to get accomplished? … We have an electronic medical record that we need to do some upgrades on. We are building a labor and delivery unit and a capital campaign to go with that. We are building a short-stay unit that, thankfully, with federal and state funding is being paid for. But there’s still work that has to be done to get that done. … [Spinning] plate No. 2 is starting to look at what are the things that we need to get done over the next five years? That starts to answer your question of what’s the capital needs that CNE has to be able to invest? … A merger is not the only way to solve that problem. … There are increasingly opportunities for health care organizations like ours to look at alliances as ways for us to be innovative about our financial platform for the next five years, including some of the capital requirements that we’re going to have.
Has anyone reached out to CNE recently [for the possibility of a merger]? No.
[caption id="attachment_434952" align="alignright" width="258"]

Dr. Michael Wagner
PBN PHOTO/DAVID HANSEN[/caption]
But does it remain a possibility? There’s the theory of it, and then there’s, “Are we in active negotiations with somebody?” I do believe there will still continue to be mergers and alliances of health care organizations coming together. I think it’s going to happen. And some people believe that for a health care organization to get to a level of stability, they have to be anywhere from $5-6 billion to $10 billion [in revenue]. Needless to say, neither Lifespan nor CNE is near those numbers … I think Rhode Island is in a challenging position because of the antitrust issues. And I think at some point, there’s going to be the need for a discussion about if we want to get to a stable health care platform in Rhode Island, how do we get there? … We don’t sit in an isolated market in Rhode Island. We have to somehow figure out how we recognize that we are living in a larger marketplace, that Rhode Island is sitting in a larger marketplace, and can enable and support the health organizations in the state to become more competitive in that larger marketplace. And right now I think that we’re at a competitive disadvantage.
What do you think it would take to get there? There’s always the dialogue … around Lifespan and Care New England coming together. Obviously, that was very much opposed by not only Attorney General [Peter F.] Neronha but also from a federal perspective. So there would have to be some kind of way to figure out how to work around that. And then the other is that CNE was in discussions with Mass General Brigham. There have been no discussions of rekindling any of this. … We are not in any active discussions with anybody around mergers, and I’ve made it very clear to the team that I do not want their time diverted … I’ve told the team: we are focused on margin and our five-year roadmap, and there are not [merger] discussions going on right now.
Let’s jump to CNE’s status in regard to staffing. We currently have 700 positions open – 130 of them are nurses. We anticipate that we’ll need to hire about 1,500 positions in 2023. We currently have 39 RN travelers [contract registered nurses who take temporary jobs in high-need areas] in the organization.
Would you consider staffing one of the main challenges? It’s certainly getting better. We’ve seen our rates come down on the traveler [nurses] side. We’ve seen some of the talent acquisition team has done a tremendous job in all sorts of tactics in terms of pushing more direct community support to build applicant flow, increasing direct touch to applicant pools through on-site career and special events, increasing targeted sponsor ads for focused roles, offering retention bonuses for select roles and leveraging select special program vendors to provide quicker talent pools for focused roles. … On the nursing side … there are two colleges here in Rhode Island that have both said that their RN programs are not filling. And it’s for two reasons. One that I thought was really shocking was that there aren’t enough RN candidates for the schools that meet the basic qualifications from a test capability perspective. … That’s concerning because that’s a pipeline issue. And then the second piece is the number of teachers and professors in nursing schools.
You mentioned earlier that you’ve met with John Fernandez, who recently started as Lifespan CEO and president. Are you going to keep that same collaborative relationship that each of your predecessors had? Yes. John and I know each other from Boston. I have a deep respect for John. I think he’s a great guy. He gets stuff done, he’s a no-nonsense guy. … We’ve developed a good working and collaborative relationship. We have to remember that Care New England and Lifespan already have very deep ties with each other. … The narrative is Care New England and Lifespan are at each other’s throats, trying to put each other out of business. The real narrative is that we already have a deep relationship, especially between Women & Infants and Rhode Island Hospital, and that there are other ways that we’ve been looking to collaborate. Around cardiology, for example: We’ve had cardiology folks at Lifespan and our folks down at Kent talking about opportunities for collaboration. And with John and I coming into the market, coming with not only a mindset of looking for ways to collaborate but our boards are incredibly supportive of us figuring out ways to collaborate with each other.